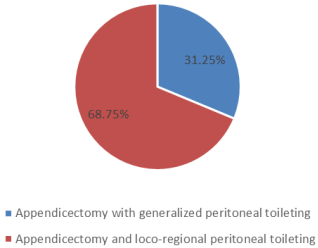
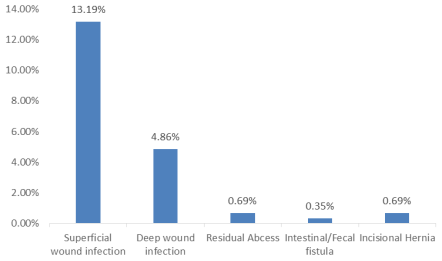
Background: Appendicular mass, a common occurrence in acute appendicitis (10% of cases), develops within 24-48 hours of symptom onset. Management strategies, including early appendectomy, non-operative management with or without drainage, and interval appendectomy, vary widely. This study aims to evaluate the outcomes of early surgical management and compare different surgical approaches. Methodology: This retroospective observational study was performed in different private and government hospital at Jamalpur, Manikgonj for a period of 8 years from January 2015 to December 2022. A total of 288 consecutive patients meeting eligibility criteria underwent open appendectomy within 24 hours of hospital admission due to appendicular lump diagnosis based on clinical or ultrasonographic findings. Two surgical techniques were employed: appendicectomy with generalized peritoneal toileting and appendicectomy with loco-regional peritoneal toileting All data were collected from hospital records. Follow-up records for a period of 2 weeks and at the end of 1 year were reviewed. Results: Patients had a mean age of 30.04 years, mostly male and under 30 years old. Appendicular lump with abscess was predominant (73.96%), along with perforated appendix and presence of pus (71.18% and 75.35% respectively). 68.75% underwent appendicectomy with loco-regional toileting, and 31.25% with generalized peritoneal toileting. Both groups were similar in demographics and perioperative findings, with common difficulties in localization and dissection (76.79% and 88.89% respectively). No bowel injuries occurred in the loco-regional toileting group. Postoperative complications were significantly lower in this group, especially superficial and deep wound infections (11.61% vs 16.67%, 2.53% vs 10%). Fecal fistula and incisional hernia were observed in the generalized peritoneal toileting group (1.11%, 2.22%). Operative time was notably shorter in the loco-regional peritoneal toileting group (92 minutes vs 65 minutes) Conclusion: Early appendicectomy allows for single-admission treatment, serving as an effective alternative to conservative therapy by significantly reducing hospital stays and expenses. Specifically, early appendicectomy with loco-regional peritoneal toileting demonstrates shorter operative times and lower post-operative complications compared to generalized peritoneal toileting, suggesting its favorable utility in managing appendicular mass and warranting further optimization in surgical strategies.
| Published in | Clinical Medicine Research (Volume 13, Issue 3) |
| DOI | 10.11648/j.cmr.20241303.12 |
| Page(s) | 33-38 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Early Surgery, Appendicular Mass, Loco-regional Peritoneal Toileting, Generalized Peritoneal Toileting, Bangladesh
Variables | Frequency (n=288) | Percentage |
|---|---|---|
Age category | ||
0-10 | 19 | 6.60 |
11-20 | 64 | 22.22 |
21-30 | 97 | 33, 68 |
31-40 | 53 | 18.40 |
41-50 | 53 | 11.46 |
>50 | 22 | 7.64 |
Gender | ||
Male | 160 | 55.56 |
Female | 128 | 44.44 |
Mean age: 30.04± 14.34 SD | ||
Diagnosis | Frequency | Percentage |
|---|---|---|
Appendicular lump | 69 | 23.96 |
Appendicular abcess | 03 | 1.04 |
Appendicular lump with abcess | 213 | 73.96 |
Appendicular lump with abcess with left ovarian cyst | 1 | 0.35 |
Appendicular lump with purulent peritonitis | 1 | 0.35 |
Appendicular lump with sloughing of Caecum | 1 | 0.35 |
Per operative Appendix condition | ||
Perforated | 205 | 71.18 |
Phlegnomous | 156 | 54.17 |
Gangrenous | 08 | 2.78 |
Presence of pus | 217 | 75.35 |
Variables | Appendicectomy and generalized peritoneal toileting (n=90) N (%) | Appendicectomy with loco-regional peritoneal toileting (n=198) N (%) | P-value |
|---|---|---|---|
Mean age ± SD | 29.04±10.12 | 31.23± 9.15 | 0.64 |
Operative findings | |||
Simple mass | 21 (23.33%) | 59 (29.80) | |
Pus collection | 60 (66.67%) | 120 (60.68) | .049 |
Appendicular abcess | 09 (10%) | 19 (9.60) | |
Operative Complication | |||
Difficulty in localization of appendix | 83 (92.22%) | 189 (95.45) | |
Difficulty in dissection | 69 (76.67%) | 176 (88.89) | |
Bleeding | 5 (5.56%) | 27 (13.64) | .071 |
Adjacent bowel injury | 01 (1.11%) | 00 (0.00) | |
Need to extend incision | 8 (8.89%) | 13 (6.57) | |
Mean Operative time (minutes) | 92 | 65 | .023 |
Post-operative complication | Appendicectomy and generalized peritoneal toileting (n=90) N (%) | Appendicectomy with loco-regional peritoneal toileting (n=198) N (%) | P-value |
|---|---|---|---|
Superficial wound infection | 15 (16.67) | 23 (11.61) | |
Deep wound infection | 09 (10) | 05 (2.53) | |
Residual Abcess | 00 (00) | 02 (1.01) | .038 |
Intestinal/Fecal fistula | 01 (1.11) | 00 (00) | |
Incisional Hernia | 02 (2.22) | 00 (00) |
STATA | Statistical Software for Data Science |
| [1] | Senapathi PSP, Bhattacharya D, Ammori BJ. Early laparoscopic appendectomy for appendicular mass. Surg Endosc Other Interv Tech. 2002; 16:1783 –5. |
| [2] | Ponsky TA, Kittle K, Eichelberger MR, Gilbert JC, Brody F, Newman KD. Hospital- and patient-level characteristics and the risk of appendiceal rupture and negative appendectomy in children. JAMA. 2004; 292:1977 –82. |
| [3] | Furuya T, Inoue M, Sugito K, Goto S, Kawashima H, Kaneda H, et al. Effectiveness of interval appendectomy after conservative treatment of pediatric ruptured appendicitis with abscess. Indian J Surg. 2015; 77:1041 –4. |
| [4] | Church JT, Klein EJ, Carr BD, Bruch SW. Early appendectomy reduces costs in children with perforated appendicitis. J Surg Res. 2017; 220: 119 –24. |
| [5] | SK, Talukdar R, Singh NK. Assessment of the relevance of interval appendicectomy in treatment of appendicular lump: a prospective study. Int J Sci Study 2016; 4: 162–6. |
| [6] | Ram KR, Chandana S, Koshti S. A study of outcome of nonoperative versus operative management in 50 cases of appendicular lump. Int Surg J 2017; 4: 2233–7. |
| [7] | Kumar CD, Abhijit S, Arupjyoti B, et al. Laparoscopic appendicectomy in appendicular lump. International Journal of Pharmaceutical Science Invention 2013; 2: 1–2. |
| [8] | Bailey H. The Ochsner-Sherren (Delayed) Treatment of acute appendicitis: Indications and technique. Br Med J 1930; 1(3603): 140-3. |
| [9] | Dhanasekharan N, Raj P, Ganeshram P, Venkatesan V. Does Ochsner-Sherren Regimen Still Hold True in the Management of Appendicular Mass? Ochsner-Sherren Rejimi Halen Apendiküler Kitle Tedavisinin Düzenlenmesinde Geçerli Midir? Ulus Travma Acil Cerrahi Derg 2010; 16(1): 43-6. |
| [10] | Russel RCG, William NS. Vermoform appendix. In: Short practice of surgery; 24th edition; (2) 2004. pp. 1203 e8. |
| [11] | Lai HW, Loong CC, chiu JH, Chau GY, Wu CW, Lui WY. Interval appendectomy after conservative treatment of an appendiceal mass. World J Surg 2006 Mar; 30:352e 7. |
| [12] | Okune G, Marek, Jaros 1aw K. Management of appendiceal mass In Children and adults: our experience. Internet J Surg 2007; 9(2). |
| [13] | Deakin DE, Ahmed I. Interval appendectomy after resolution of adult inflammatory appendix masseis it necessary? Surgeon 2007; 5(1): 45e 50. |
| [14] | Kim JK, Ryoo S, Oh HK, et al. Management of appendicitis presenting with abscess or mass. J Korean Soc Coloproctol 2010; 26(6): 413-419. |
| [15] | Tannoury J, Abboud B. Treatment options of inflammatory appendiceal masses in adults. World J Gastroenterol 2013; 19(25): 3942-3950. |
| [16] | Patel BJ, Patel KH. A comparative study of appendicular lump management. Int Surg J 2015; 2(2): 235-238. |
| [17] | Gilkar IA, Mushtaq U, Peer JA, et al. Management of appendicular lump at tertiary care hospital. J. Evid. Based Med. Healthc.2019; 6(3), 135-138. |
| [18] | Rahman, M. A. M., Chowdhury, T. K., Chowdhury, M. Z. et al. Early appendectomy for appendicular mass: operative findings and outcome in 220 children—a developing country perspective. Ann Pediatr Surg 16, 39 (2020). |
| [19] |
Bahram MA. Evaluation of early surgical management of complicated appendicitis by appendicular mass. Int J Surg. 2011; 9(1): 101-3.
https://doi.org/10.1016/j.ijsu.2010.10.006 Epub 2010 Oct 20. PMID: 20965290. |
| [20] | Garba ES, Ahmed A. Management of appendiceal mass. Ann Afr Med 2008; 7(4): 200-204. |
| [21] | Corfield L. Interval appendicectomy after appendiceal mass or abscess in adults: what is “best practice”? Surg Today 2007; 37(1): 1-4. |
| [22] | Ali M, Jahan KI. Early appendicectomy in appendicular massreview of literature. Journal of Surgical Science 2016; 20(1): 3335. |
| [23] | Ali Khan S, Ali M, Seerat MI. Efficacy of early exploration in appendicular mass. Pakistan Journal of Medical & Health Sciences 2016; 10(3): 781-3. 674. |
| [24] | Arshad M, Aziz LA, Qasim M, Altaf K, Talpur H. Early appendicectomy in appendicular mass--a Liaquat University Hospital experience. J Ayub Med Coll Abbottabad 2008; 20(1): 70-2. |
APA Style
Sarwar, J. M., Shamsuddin, A. K. M., Munira, S. (2024). Early Surgical Management of Appendicular Mass: Evaluation of Surgical Outcome in Selected Private and Government Hospitals, Bangladesh. Clinical Medicine Research, 13(3), 33-38. https://doi.org/10.11648/j.cmr.20241303.12
ACS Style
Sarwar, J. M.; Shamsuddin, A. K. M.; Munira, S. Early Surgical Management of Appendicular Mass: Evaluation of Surgical Outcome in Selected Private and Government Hospitals, Bangladesh. Clin. Med. Res. 2024, 13(3), 33-38. doi: 10.11648/j.cmr.20241303.12
AMA Style
Sarwar JM, Shamsuddin AKM, Munira S. Early Surgical Management of Appendicular Mass: Evaluation of Surgical Outcome in Selected Private and Government Hospitals, Bangladesh. Clin Med Res. 2024;13(3):33-38. doi: 10.11648/j.cmr.20241303.12
@article{10.11648/j.cmr.20241303.12,
author = {Jahangir Md Sarwar and Abul Kalam Md Shamsuddin and Sirajam Munira},
title = {Early Surgical Management of Appendicular Mass: Evaluation of Surgical Outcome in Selected Private and Government Hospitals, Bangladesh
},
journal = {Clinical Medicine Research},
volume = {13},
number = {3},
pages = {33-38},
doi = {10.11648/j.cmr.20241303.12},
url = {https://doi.org/10.11648/j.cmr.20241303.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20241303.12},
abstract = {Background: Appendicular mass, a common occurrence in acute appendicitis (10% of cases), develops within 24-48 hours of symptom onset. Management strategies, including early appendectomy, non-operative management with or without drainage, and interval appendectomy, vary widely. This study aims to evaluate the outcomes of early surgical management and compare different surgical approaches. Methodology: This retroospective observational study was performed in different private and government hospital at Jamalpur, Manikgonj for a period of 8 years from January 2015 to December 2022. A total of 288 consecutive patients meeting eligibility criteria underwent open appendectomy within 24 hours of hospital admission due to appendicular lump diagnosis based on clinical or ultrasonographic findings. Two surgical techniques were employed: appendicectomy with generalized peritoneal toileting and appendicectomy with loco-regional peritoneal toileting All data were collected from hospital records. Follow-up records for a period of 2 weeks and at the end of 1 year were reviewed. Results: Patients had a mean age of 30.04 years, mostly male and under 30 years old. Appendicular lump with abscess was predominant (73.96%), along with perforated appendix and presence of pus (71.18% and 75.35% respectively). 68.75% underwent appendicectomy with loco-regional toileting, and 31.25% with generalized peritoneal toileting. Both groups were similar in demographics and perioperative findings, with common difficulties in localization and dissection (76.79% and 88.89% respectively). No bowel injuries occurred in the loco-regional toileting group. Postoperative complications were significantly lower in this group, especially superficial and deep wound infections (11.61% vs 16.67%, 2.53% vs 10%). Fecal fistula and incisional hernia were observed in the generalized peritoneal toileting group (1.11%, 2.22%). Operative time was notably shorter in the loco-regional peritoneal toileting group (92 minutes vs 65 minutes) Conclusion: Early appendicectomy allows for single-admission treatment, serving as an effective alternative to conservative therapy by significantly reducing hospital stays and expenses. Specifically, early appendicectomy with loco-regional peritoneal toileting demonstrates shorter operative times and lower post-operative complications compared to generalized peritoneal toileting, suggesting its favorable utility in managing appendicular mass and warranting further optimization in surgical strategies.
},
year = {2024}
}
TY - JOUR T1 - Early Surgical Management of Appendicular Mass: Evaluation of Surgical Outcome in Selected Private and Government Hospitals, Bangladesh AU - Jahangir Md Sarwar AU - Abul Kalam Md Shamsuddin AU - Sirajam Munira Y1 - 2024/06/19 PY - 2024 N1 - https://doi.org/10.11648/j.cmr.20241303.12 DO - 10.11648/j.cmr.20241303.12 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 33 EP - 38 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20241303.12 AB - Background: Appendicular mass, a common occurrence in acute appendicitis (10% of cases), develops within 24-48 hours of symptom onset. Management strategies, including early appendectomy, non-operative management with or without drainage, and interval appendectomy, vary widely. This study aims to evaluate the outcomes of early surgical management and compare different surgical approaches. Methodology: This retroospective observational study was performed in different private and government hospital at Jamalpur, Manikgonj for a period of 8 years from January 2015 to December 2022. A total of 288 consecutive patients meeting eligibility criteria underwent open appendectomy within 24 hours of hospital admission due to appendicular lump diagnosis based on clinical or ultrasonographic findings. Two surgical techniques were employed: appendicectomy with generalized peritoneal toileting and appendicectomy with loco-regional peritoneal toileting All data were collected from hospital records. Follow-up records for a period of 2 weeks and at the end of 1 year were reviewed. Results: Patients had a mean age of 30.04 years, mostly male and under 30 years old. Appendicular lump with abscess was predominant (73.96%), along with perforated appendix and presence of pus (71.18% and 75.35% respectively). 68.75% underwent appendicectomy with loco-regional toileting, and 31.25% with generalized peritoneal toileting. Both groups were similar in demographics and perioperative findings, with common difficulties in localization and dissection (76.79% and 88.89% respectively). No bowel injuries occurred in the loco-regional toileting group. Postoperative complications were significantly lower in this group, especially superficial and deep wound infections (11.61% vs 16.67%, 2.53% vs 10%). Fecal fistula and incisional hernia were observed in the generalized peritoneal toileting group (1.11%, 2.22%). Operative time was notably shorter in the loco-regional peritoneal toileting group (92 minutes vs 65 minutes) Conclusion: Early appendicectomy allows for single-admission treatment, serving as an effective alternative to conservative therapy by significantly reducing hospital stays and expenses. Specifically, early appendicectomy with loco-regional peritoneal toileting demonstrates shorter operative times and lower post-operative complications compared to generalized peritoneal toileting, suggesting its favorable utility in managing appendicular mass and warranting further optimization in surgical strategies. VL - 13 IS - 3 ER -
Sheikh Russel National Gastroliver Institute and Hospital, Dhaka, Bangladesh
Sheikh Russel National Gastroliver Institute and Hospital, Dhaka, Bangladesh
Sheikh Russel National Gastroliver Institute and Hospital, Dhaka, Bangladesh