Consultation for mechanical bowel obstruction is one of the most common reasons in emergency and surgical departments. Transmural hernia of the strangulated uterus after myomectomy is a rare etiology of intestinal obstruction. Their diagnosis is increasingly complex and is discovered during an exploratory laparotomy. In this observation, we report the case of this 34-year-old patient with a history of myomectomy, nulliparous admitted for persistent abdominal pain and vomiting. an abdominopelvic ultrasound showed images of uterine myomas in necrobiosis. the patient presented an occlusive syndrome for which an abdominopelvic MRI which confirmed the diagnosis of aseptic necrobiosis. This unusual image mimicking that of a necrobiosis of uterine myoma was the difficulty which allowed this diagnostic error and the delay in the treatment of this patient. As this philosophy emphasizes (never let the sun rise or set in case of mechanical obstruction of the small intestine). Given the persistence of clinical signs, an abdominal CT scan was requested and confirmed the diagnosis of occlusive syndrome. conclusion: Faced with the diagnosis of an acute intestinal obstruction following a myomectomy by a combination of persistent abdominal pain, vomiting, cessation of materials and gas, systematically look for an obstruction of internal hernia by incarceration in a myomectomy cubicle. Exploratory laparotomy makes it possible to find the etiology and treat it.
| Published in | Clinical Medicine Research (Volume 13, Issue 3) |
| DOI | 10.11648/j.cmr.20241303.11 |
| Page(s) | 29-32 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Transmural Hernia, Intestinal Obstruction, Aseptic Necrobiosis
CHU | Centre Hospitalier Universitaire |
| [1] | Mathias J, Phi I, Bruot O, Ganne PA, Laurent V, Regent D. Internal hernias. EMC - Radiology and Medical Imaging - Abdominal - Digestive. Jan 2008; 3(4): 1-8. |
| [2] | Meyers, MA. Dynamic radiology of the abdomen: normal and pathological anatomy, 4th ed. New York, NY: Springer Verlag, 1994 Google Scholar. |
| [3] | Fadil A. Acute intestinal obstruction by incarceration of the small intestine in the broad ligament: a case report. 8 Jul 2021 [cited 28 Mar 2023]. |
| [4] | F. N. Koksoy, G. R. Soybir, T. M. Bulut, O. Yalcin, Y. Aker, H. Kose, Internal supravesical hernia: report of a case, Am. Surg. 61(11) (1995) 1023-1024. |
| [5] | I. Sozen, J. Nobel, Inguinal mass due to an external supravesical hernia and acute abdomen due to an internal supravesical hernia: a case report and review of the literature, Hernia 8(4) (2004) 389-392. |
| [6] | M. Cisse, I. Konate, O. Ka, M. Dieng, A. Dia, C. T. Toure, Internal supravesical hernia as a rare cause of intestinal obstruction: a case report, J. Med. Case Rep. 3(2009). |
| [7] | T. Watanabe, M. Kamiga, I. Hirai, M. Mizutani, A. Fuse, W. Kimura, A case of supravesical hernia, Nihon Geka Gakkai Zasshi 65(3) (2004) 801-805. |
| [8] | Hoeffel JC, Zimberger J, Pocard B, Hoeffel C. Demonstration by computed tomography of a case of internal small bowel herniation. BJR. nov 1992; 65(779): 1045-6. |
| [9] | Bedioui H, Daghfous A, Daghfous A, Ksantini R, Nouira K, Chebbi F, et al. Internal falciform ligament hernia revealed by acute intestinal obstruction. La Presse Médicale. Jan 1, 2008; 37(1, Part 1): 44-7. |
| [10] | T. Sato, K. Miyagawa, N. Sakamoto, A case of internal supravesical hernia, Nihon Rinsho Geka Gakkai Zasshi 68(3) (2007) 706-709. |
| [11] | K. Asanuma, M. Yoshida, S. Takanashi, M. Kashiyama, M. Ishigo-Oka, H. Kawashima, A case of internal supravesical hernia repaired by laparoscopic surgery, Nihon Rinsho Geka Gakkai Zasshi 74(1) (2013) 238-242. |
| [12] | Zarvan NP, Lee FT Jr, Yandow DR, Unger JS. Abdominal hernias: results of computed tomography. AJR, 1995; 164: 1391-1395. |
| [13] | Blachar A, Federle MP. Bowel obstruction after liver transplantation: clinical and CT findings in 48 cases with emphasis on internal herniation. Radiology 2001; 218: 384-388. |
| [14] | Jeremy B, Bonneau C, Guillo E, Paniel BJ, Le Tohic A, Haddad B, et al. Transmural isthmic hernia of the uterus: results of isthmorraphy on symptomatology and fertility. Gynecology Obstetrics & Fertility. Oct 1, 2013; 41(10): 588-96. |
| [15] | Ghahremani GG. Abdominal and pelvic hernias. In: Gore RM, Levine MS, eds. Handbook of Gastrointestinal Radiology, 2nd ed. Philadelphia, Pennsylvania: Saunders, 1994. |
| [16] |
Masuda H, Uchida H, Maruyama T, Sato K, Sato S, Tanaka M. Successful treatment of atypical cesarean scar defect using endoscopic surgery. BMC Pregnancy Childbirth. 2015 Dec 22; 15: 342.
https://doi.org/10.1186/s12884-015-0730-x PMID: 26696492; PMCID: PMC4687144. |
| [17] | Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology 2001; 218: 68-74 Google Scholar. |
| [18] | Hong, Seong Sook M. D.; Kim, Ah Jeune, M. D.; Kim, Pyo Nyun M. D.; Lee, Moon-Gyu MD; Ha, Hyun Kwon MD. Current diagnostic role of CT in the evaluation of internal hernia. Journal of computed tomography 29(5): p 604-609, September 2005. | |
| [19] | R Zissin, M Hertz, G Gayer, H Paran, A Osadchy, Congenital internal hernia as a cause of small bowel obstruction: CT findings in 11 adult patients, British Journal of Radiology, Volume 78, Issue 933, 1 September 2005, Pages 796-802, |
| [20] | Haku T, Daidouji K, Kawamura H et al: Internal hernia by a defect of the broad ligament of the uterus. Abdom Imagerie 2004; 29: 161-163. |
| [21] |
Akyildiz H, Artis T, Sozuer E, Akcan A, Kucuk C, Sensoy E, Karahan I. Internal hernia: complex diagnostic and therapeutic problem. Int J Surg. 2009 Aug; 7(4): 334-7.
https://doi.org/10.1016/j.ijsu.2009.04.013 Epub 2009 May 5. PMID: 19422936. |
| [22] |
Masson E. EM-Consulte. [cited March 28, 2023]. Diagnosis and management of uterine perforation by intrauterine device: from 11 cases. Available at:
https://www.em-consulte.com/article/810124/diagnostic-et-prise-en-charge-des-perforations-ute |
| [23] | Traoré H. Uterine perforation intestinal occlusion small bowel incarceration l'hôpital Nianankoro FOMBA de Ségou. 2022 [cited 28 March 2023]; Available from: |
| [24] | Harbin WP. Tomographic diagnosis of internal hernia. Radiology 1982; 143: 736 PubMed Google Scholar. |
| [25] | Sasaya T, Yamaguchi A, Isogai M, Harada T, Kaneoka Y, Suzuki M. Supravesical hernia: diagnosis by computed tomography. Abdom Imagerie 2001; 26: 89-91 Google Scholar. |
APA Style
Mamadouba, C., Romuald, B. P., Fodé, C., Mamadou, C. (2024). Strangulated Transmural Hernia of the Uterus After Myomectomy: A Rare Cause of Bowel Obstruction. Clinical Medicine Research, 13(3), 29-32. https://doi.org/10.11648/j.cmr.20241303.11
ACS Style
Mamadouba, C.; Romuald, B. P.; Fodé, C.; Mamadou, C. Strangulated Transmural Hernia of the Uterus After Myomectomy: A Rare Cause of Bowel Obstruction. Clin. Med. Res. 2024, 13(3), 29-32. doi: 10.11648/j.cmr.20241303.11
AMA Style
Mamadouba C, Romuald BP, Fodé C, Mamadou C. Strangulated Transmural Hernia of the Uterus After Myomectomy: A Rare Cause of Bowel Obstruction. Clin Med Res. 2024;13(3):29-32. doi: 10.11648/j.cmr.20241303.11
@article{10.11648/j.cmr.20241303.11,
author = {Camara Mamadouba and Bly Persédoué Romuald and Cissé Fodé and Camara Mamadou},
title = {Strangulated Transmural Hernia of the Uterus After Myomectomy: A Rare Cause of Bowel Obstruction
},
journal = {Clinical Medicine Research},
volume = {13},
number = {3},
pages = {29-32},
doi = {10.11648/j.cmr.20241303.11},
url = {https://doi.org/10.11648/j.cmr.20241303.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20241303.11},
abstract = {Consultation for mechanical bowel obstruction is one of the most common reasons in emergency and surgical departments. Transmural hernia of the strangulated uterus after myomectomy is a rare etiology of intestinal obstruction. Their diagnosis is increasingly complex and is discovered during an exploratory laparotomy. In this observation, we report the case of this 34-year-old patient with a history of myomectomy, nulliparous admitted for persistent abdominal pain and vomiting. an abdominopelvic ultrasound showed images of uterine myomas in necrobiosis. the patient presented an occlusive syndrome for which an abdominopelvic MRI which confirmed the diagnosis of aseptic necrobiosis. This unusual image mimicking that of a necrobiosis of uterine myoma was the difficulty which allowed this diagnostic error and the delay in the treatment of this patient. As this philosophy emphasizes (never let the sun rise or set in case of mechanical obstruction of the small intestine). Given the persistence of clinical signs, an abdominal CT scan was requested and confirmed the diagnosis of occlusive syndrome. conclusion: Faced with the diagnosis of an acute intestinal obstruction following a myomectomy by a combination of persistent abdominal pain, vomiting, cessation of materials and gas, systematically look for an obstruction of internal hernia by incarceration in a myomectomy cubicle. Exploratory laparotomy makes it possible to find the etiology and treat it.
},
year = {2024}
}
TY - JOUR T1 - Strangulated Transmural Hernia of the Uterus After Myomectomy: A Rare Cause of Bowel Obstruction AU - Camara Mamadouba AU - Bly Persédoué Romuald AU - Cissé Fodé AU - Camara Mamadou Y1 - 2024/05/30 PY - 2024 N1 - https://doi.org/10.11648/j.cmr.20241303.11 DO - 10.11648/j.cmr.20241303.11 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 29 EP - 32 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20241303.11 AB - Consultation for mechanical bowel obstruction is one of the most common reasons in emergency and surgical departments. Transmural hernia of the strangulated uterus after myomectomy is a rare etiology of intestinal obstruction. Their diagnosis is increasingly complex and is discovered during an exploratory laparotomy. In this observation, we report the case of this 34-year-old patient with a history of myomectomy, nulliparous admitted for persistent abdominal pain and vomiting. an abdominopelvic ultrasound showed images of uterine myomas in necrobiosis. the patient presented an occlusive syndrome for which an abdominopelvic MRI which confirmed the diagnosis of aseptic necrobiosis. This unusual image mimicking that of a necrobiosis of uterine myoma was the difficulty which allowed this diagnostic error and the delay in the treatment of this patient. As this philosophy emphasizes (never let the sun rise or set in case of mechanical obstruction of the small intestine). Given the persistence of clinical signs, an abdominal CT scan was requested and confirmed the diagnosis of occlusive syndrome. conclusion: Faced with the diagnosis of an acute intestinal obstruction following a myomectomy by a combination of persistent abdominal pain, vomiting, cessation of materials and gas, systematically look for an obstruction of internal hernia by incarceration in a myomectomy cubicle. Exploratory laparotomy makes it possible to find the etiology and treat it. VL - 13 IS - 3 ER -
Farah Polyclinic, Abidjan, Ivory Coast
Department of General Surgery, Centre Hospitalier Universitaire Treichville, Abidjan, Côte D'Ivoire
Farah Polyclinic, Abidjan, Ivory Coast
Department of General Surgery, Centre Hospitalier Universitaire Treichville, Abidjan, Côte D'Ivoire

Figure 1. A- Coronal section of pelvic MRI showing a necrobitic uterine myoma; B- sagittal section: Respect for the uterine cavity with an image confused with a necrotic myoma.
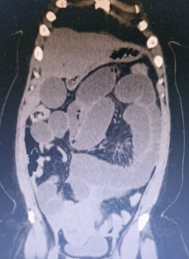
Figure 2. Abdominal-pelvic CT scan, coronal section: distension of the gallbladder with a transition zone at pelvic level.
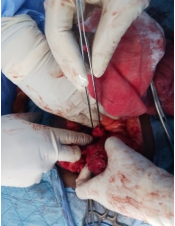
Figure 3. Uterine breach of isthmic seat after disincarceration of the ileal loop.

